TMJ Physiotherapy: How Physio Helps Jaw Pain
Jaw pain, clicking, and limited opening are common, and most cases are not a dental problem. Manual therapy and jaw exercise are an evidence-based first-line option for temporomandibular disorders, and the neck is involved more often than people expect.
BY SANAZ DAVARIAN, PHD
Quick answer. Most jaw pain is not a dental problem. Temporomandibular disorder (TMD) is pain and dysfunction at the jaw joint and the muscles that move it, and the common muscular and joint types respond to physiotherapy. Manual therapy and therapeutic exercise are the most consistently supported approaches in the research, with a moderate effect on both pain and how wide you can open. The piece that gets missed is the neck: the upper cervical spine and the jaw share muscles, nerves, and load, so jaw treatment that ignores the neck often underperforms. When grinding, occlusion, or a tooth is the driver, a dentist is still part of the plan, and physiotherapy works alongside dental care rather than instead of it.
Most jaw pain is not a dental problem. Temporomandibular disorder (TMD) affects the jaw joint and the muscles that move it, and the common muscular and joint types often respond well to physiotherapy. Manual therapy and therapeutic exercise are the most consistently supported approaches in the research, with moderate effects on pain and jaw opening. One area that is frequently overlooked is the neck: the upper cervical spine shares muscles and nerves with the jaw, so jaw treatment that ignores the neck may underperform. At Medstar Sport Physio in North Vancouver, assessment includes both the jaw and the neck. When grinding or a bite issue is involved, dental care and physiotherapy work alongside each other. What the right combination looks like depends on the type of TMD identified at your first visit.
If your jaw aches with chewing, clicks when you open, or feels tight and tired by the end of a screen-heavy day, that is the pattern this article describes.
What TMD actually is
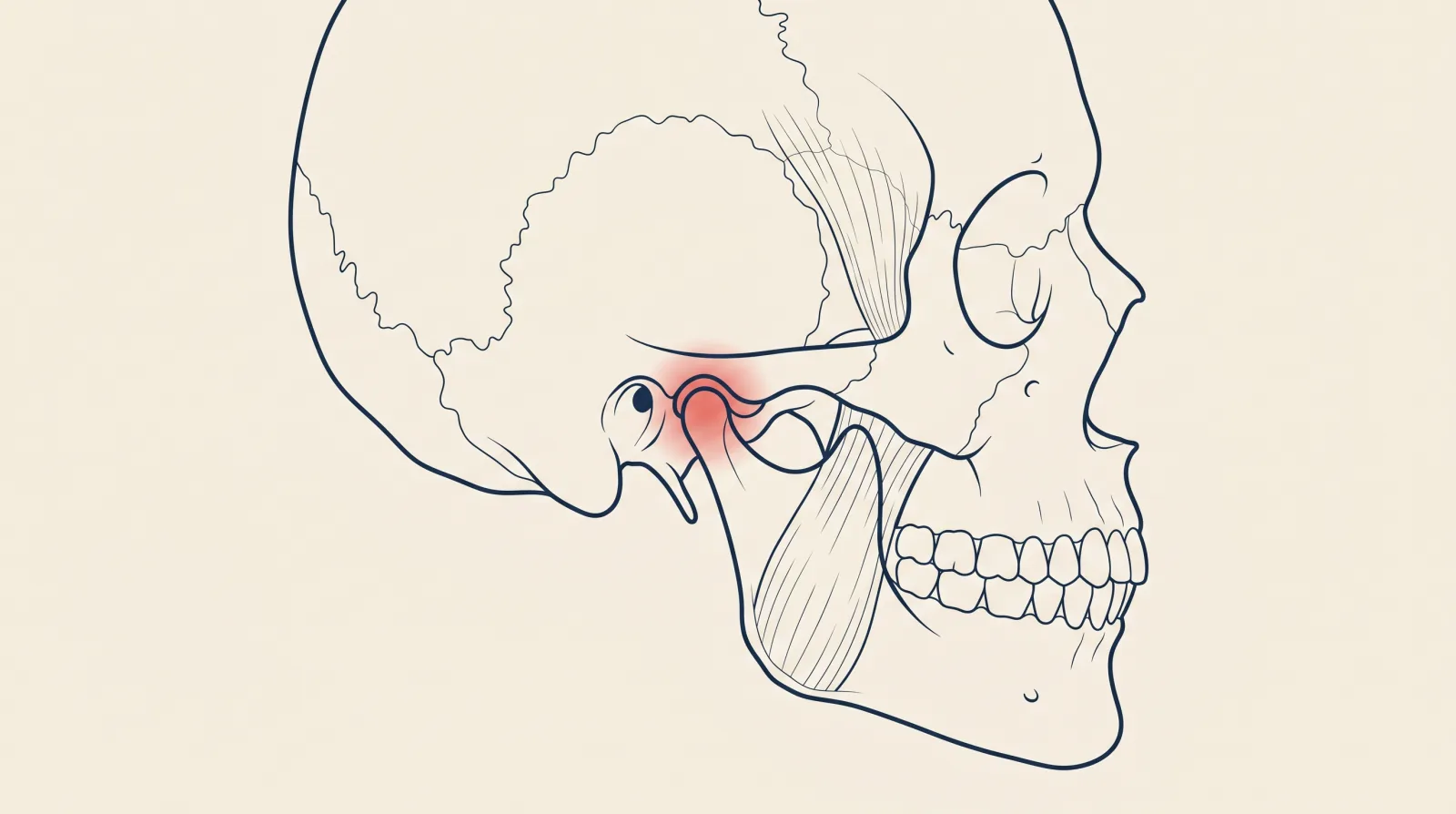
The temporomandibular joint (TMJ) is the hinge just in front of each ear where the lower jaw meets the skull. It is a working joint with a cartilage disc, a capsule, and a set of muscles that close and move the jaw — the masseter over the cheek and the temporalis at the temple are the two you can feel. "TMD" is the umbrella term for pain and dysfunction in this system. It usually sorts into a few overlapping types: a muscular type (the chewing muscles are overloaded and tender), a joint type (the joint itself is irritated), and a disc type (the cartilage disc clicks or catches as the jaw moves).
The everyday presentation is familiar. Jaw pain with chewing, a click or a catch when opening, a feeling of tightness or fatigue in the jaw, headaches near the temples, and sometimes a limited opening — not quite enough to bite into a thick sandwich. Most cases are muscular or mixed, which is the group physiotherapy helps most.
What the evidence says about physiotherapy for TMD
Physiotherapy for TMD is not a fringe idea — it is a well-studied, first-line conservative option. An umbrella review of systematic reviews in the Journal of Clinical Medicine found moderate effects for manual therapy and therapeutic exercise on both pain intensity and maximum mouth opening, with the strongest single-modality effect reported for low-level laser therapy. A systematic review of exercise therapy in Frontiers in Oral Health reached a similar conclusion for jaw exercise specifically, and a broader systematic review of physiotherapy for TMD found physiotherapy generally superior to no treatment and at least comparable to other conservative options.
Two honest caveats run through this literature. The studies are heterogeneous and many are small, so the certainty of evidence is limited to moderate. And the benefit is clearest in the short term. That matches what conservative care is for: settling the pain, restoring movement, and giving you the self-management tools to keep it settled. In practice the treatment is unglamorous — hands-on work to the jaw and neck muscles, graded jaw movement and control exercises, and education on the habits that load the system.
The neck connection most jaw treatment misses
The jaw does not work in isolation. The upper cervical spine refers pain into the jaw and face, and the muscles and nerves of the neck and jaw are closely linked. A stiff, irritable upper neck can drive jaw symptoms, and a loaded jaw can feed neck and temple headaches. This is why a thorough jaw assessment always includes the neck, and why treating one without the other often leaves a stubborn case half-solved.
This is also where the local pattern shows up. On the North Shore we see a lot of desk and screen workers — people commuting in on the SeaBus to downtown offices, or working from home offices in Lonsdale and Lynn Valley — who spend the day with the head forward, the neck loaded, and the jaw quietly clenched through deadlines. Jaw pain, tension headaches, and a tight upper neck arrive together because they are loaded together. Sorting the jaw means sorting the posture and the neck that come with it. Our conditions guide to TMJ and the physiotherapy service page cover how we approach the combined picture.
What a first TMJ visit looks like at Medstar
A first jaw assessment is one part screening and one part planning. The physiotherapist takes a history — when it started, what aggravates it, whether you grind or clench, any recent dental work or trauma — and then examines the system: the jaw muscles, the joint and its movement, how far and how evenly you can open, and the upper neck. The goal of that first visit is to identify which type of TMD is driving your symptoms and to rule out the features that point somewhere else.
From there the plan is built around your findings. It usually combines hands-on treatment to the jaw and neck muscles, specific jaw movement and control exercises you continue at home, and practical changes to the habits that overload the joint — clenching awareness, desk setup, and managing the neck. For muscular jaw pain with trigger points in the masseter or temporalis, intramuscular stimulation (IMS / dry needling) is one tool a certified physiotherapist may use within scope. Between-visit work does most of the lifting, so the home program is not an afterthought.
When it is not just physiotherapy
Physiotherapy and dentistry are not competitors for jaw pain — they cover different parts of the problem. A dentist is the right call when the driver is grinding that needs a night guard, an occlusion or bite issue, or a tooth source. A physiotherapist is the right call for the muscular and joint pain, the stiffness, the limited opening, and the neck contribution. For someone who both grinds and has muscular jaw pain, the strongest outcomes use both: the guard manages the load on the teeth, the physiotherapy settles the muscles and joint. We coordinate with your dentist where that is the sensible path.
If your jaw pain followed a car crash, it is part of your ICBC claim and covered under Enhanced Care within physiotherapy — our guide to jaw and TMJ pain after a crash covers how that works.
Red flags — when to get medical or dental care first
Most jaw pain is benign and conservative care is appropriate. A few features change the plan and warrant prompt medical or dental assessment rather than a physiotherapy booking:
- A jaw that locks open or locked closed and will not move.
- Jaw pain after a direct blow or trauma, or with a tooth or facial injury.
- Significant facial swelling, fever, or a clearly tooth-related pain.
- New jaw pain with chest pain or shortness of breath, which can rarely be referred cardiac pain and is a reason to call 911 or attend Lions Gate Hospital.
In the absence of those, the path is straightforward: an assessment to identify the type, a short course of manual therapy and exercise, and a self-management plan. The strongest outcomes happen when you start before the pattern becomes long-standing.
This article is general education about temporomandibular disorders and physiotherapy. It is not personal medical or dental advice. A regulated practitioner can confirm whether the patterns described apply to you, identify the type of TMD, and coordinate with your dentist where appropriate.
Sources
- Idáñez-Robledo et al. — Effects of Physiotherapy on Pain and Mouth Opening in Temporomandibular Disorders: An Umbrella and Mapping Systematic Review with Meta-Meta-Analysis, Journal of Clinical Medicine
- Systematic review of exercise therapy for pain-related temporomandibular disorders, Frontiers in Oral Health
- Effectiveness of physiotherapy for temporomandibular disorders: a systematic review of pain and functional outcomes, Scandinavian Journal of Pain
- College of Physical Therapists of BC (CPTBC)
Share this post
Copies a ready-to-publish LinkedIn post to your clipboard and opens the LinkedIn share dialog. Paste the text into the composer and publish.

Written by
Sanaz Davarian, PhDDr. Sanaz Davarian — Registered Physiotherapist with a PhD and 20+ years of experience. Certified IMS Therapist, former Assistant Professor of Physiotherapy. North Vancouver.
This article is for general information only and does not constitute medical advice, diagnosis, or treatment. Individual presentations vary — assessment findings and treatment plans differ from person to person. If you are experiencing severe symptoms, neurological changes (numbness, weakness, bowel or bladder changes), or a significant trauma, contact your physician or emergency services. Care at Medstar Sport Physio & Health is provided by practitioners registered with their respective British Columbia regulatory colleges.
Filed under
- tmj
- jaw-pain
- temporomandibular-disorder
- headaches
- north-vancouver


