Sciatica: When It's a Disc, When It's Referred, and Why It Matters
Sciatica is one of the most misused words in back pain. Telling true nerve-root pain from referred pain changes what helps, and most leg pain settles without surgery.
BY SANAZ DAVARIAN, PHD
Few words in back pain are used as loosely as sciatica. People reach for it to describe almost any pain that travels into the leg. But the term has a specific meaning, and telling true sciatica from the look-alikes changes what actually helps. The good news running through all of it is that most of this pain settles without surgery.
What sciatica actually means
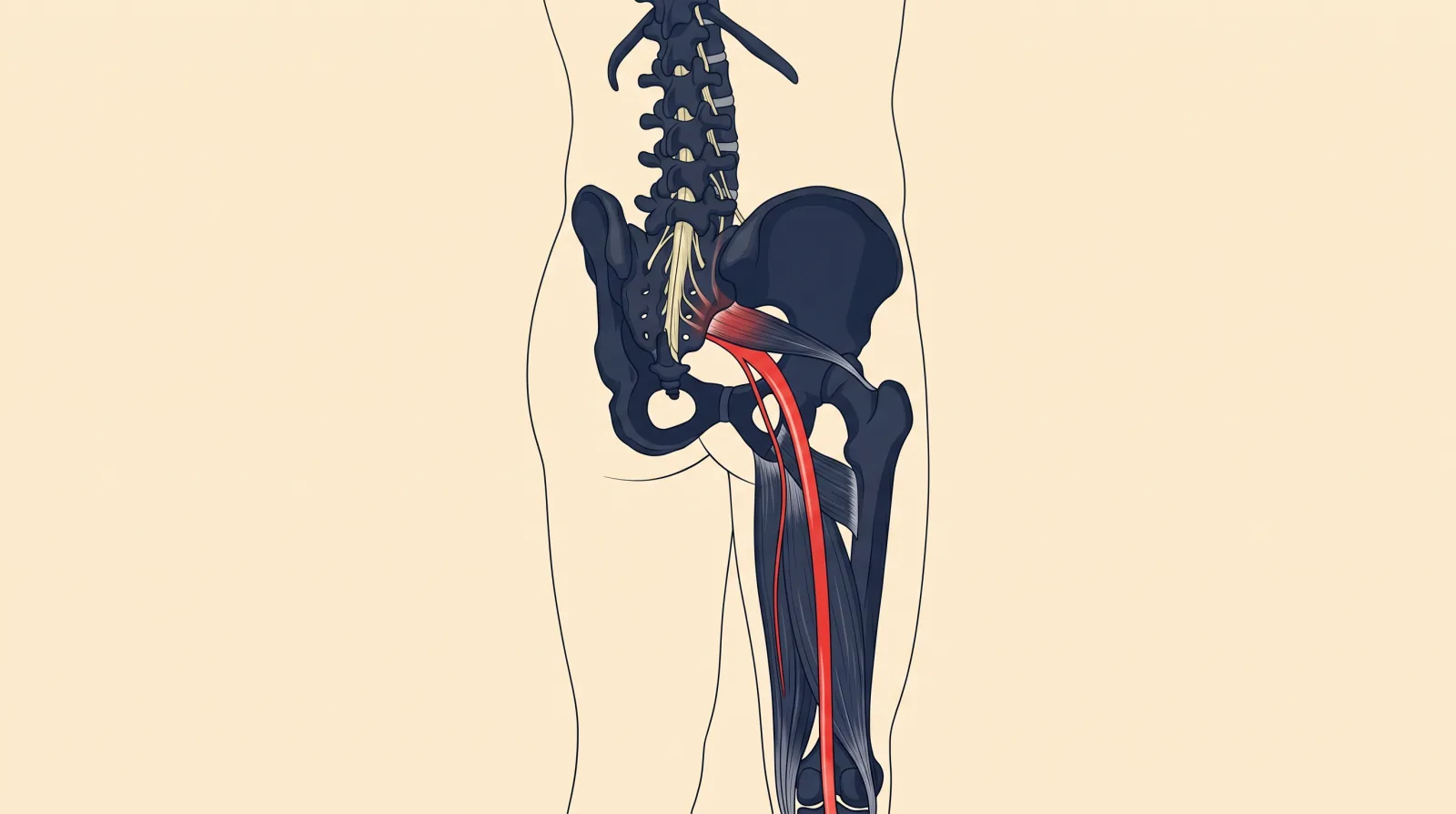
True sciatica is irritation or compression of a nerve root in the lower back, most often producing sharp, shooting, or burning pain that follows a defined path down the leg, sometimes with pins and needles, numbness, or weakness. The classic cause is a disc bulge pressing on or irritating the nerve where it exits the spine, which is why sciatica and disc involvement are so closely linked.
But not all leg pain from the back is nerve-root pain. A large share of it is referred pain, an ache that spreads from back structures or the deep buttock muscles into the thigh and sometimes lower. It can feel like it is travelling down the leg, but it is not the nerve root being compressed. The difference is not academic, because the two respond to different approaches.
How we tell them apart
At assessment, we look at the quality and distribution of the pain, how it behaves with movement, and whether there are true nerve signs. True nerve-root pain tends to follow a recognizable path, may come with numbness or weakness in a specific pattern, and often responds to particular positions or movements that change the load on the nerve. Referred pain is usually more diffuse, lacks the clear nerve signs, and tracks more with back and hip movement than with nerve tension.
This is the same careful sorting we apply across back-related leg pain, including nerve-root impingement and broader low back pain. Getting the category right is what lets us choose the right plan rather than treating every leg pain the same way.
Why an MRI usually is not the first step
People often assume sciatica means they need a scan. For most cases, an MRI does not change the early plan. The standard approach for leg pain from the back is to stay as active as the pain allows and let symptoms settle with guided care, and imaging does not alter that. We cover the broader logic in our piece on when MRI is actually needed for low back pain.
Scanning too early has a real downside. MRIs routinely show disc bulges and age-related changes in people with no pain at all, so an early scan often finds something that looks alarming but is not actually the source of the trouble. That can lead to fear, unnecessary worry, and sometimes treatment aimed at a finding that was never the problem.
Imaging earns its place when there are red-flag features, when severe symptoms are not improving over a reasonable timeframe, or when surgery is genuinely being considered.
Most of it settles without surgery
This is the reassuring core of the topic. A large share of disc-related nerve pain improves over weeks to a few months without surgery, even when a scan shows a disc bulge. Discs can reabsorb over time, and the nerve sensitivity settles as the irritation calms. Staying active within your limits, avoiding prolonged bed rest, and following a guided program gives the best chance of a good recovery.
Surgery is reserved for cases that do not improve over time despite good conservative care, or that have specific features such as significant progressive weakness. It is the exception, not the default.
What physiotherapy does
For true nerve-root pain, treatment focuses on reducing the nerve's sensitivity. That can include specific movements or positions that ease the load on the nerve, guidance on staying active in ways that do not flare it, and graded loading as symptoms settle. The aim is to keep you moving while the nerve calms, then rebuild your capacity to load the back and leg normally.
For referred pain, we address the back and hip structures driving it, restoring movement and building strength and tolerance. In both cases, the through-line is the same: keep moving, reduce sensitivity, and rebuild capacity, rather than waiting passively for the pain to disappear.
The red flags that do not wait
Most sciatica is not dangerous, but a few features need urgent care. Seek immediate medical attention if you develop numbness around the groin or buttocks, loss of bladder or bowel control, or rapidly worsening weakness in the leg. These can signal a serious condition called cauda equina syndrome, which is a surgical emergency. Significant or progressive leg weakness, even without those other features, also warrants prompt assessment.
These are uncommon, but they are the reason we always screen for them, and the reason we tell people clearly what to watch for.
When to get it assessed
If you have leg pain coming from your back, an assessment sorts true nerve-root pain from referred pain, rules out the red flags, and gives you a clear plan to settle it, usually without imaging and almost always without surgery. The most common mistake is lying still and waiting, which tends to leave you stiffer and more deconditioned.
Book a 30-minute appointment and we will work out what is actually driving your leg pain and build a plan to calm it and get you moving again.
This article is general information about sciatica and back-related leg pain. It is not personal medical advice. A regulated practitioner can confirm whether the patterns described apply to you, and the red-flag features described require urgent medical attention.
Sources
- North American Spine Society — Evidence-Based Clinical Guidelines for Lumbar Disc Herniation with Radiculopathy (2012)
- Chiu et al. — The probability of spontaneous regression of lumbar herniated disc: a systematic review, Clinical Rehabilitation (2015)
- College of Physical Therapists of BC (CPTBC)
Share this post
Copies a ready-to-publish LinkedIn post to your clipboard and opens the LinkedIn share dialog. Paste the text into the composer and publish.

Written by
Sanaz Davarian, PhDDr. Sanaz Davarian — Registered Physiotherapist with a PhD and 20+ years of experience. Certified IMS Therapist, former Assistant Professor of Physiotherapy. North Vancouver.
Filed under
- sciatica
- low-back-pain
- nerve-pain
- disc
- north-vancouver


