First-Time Shoulder Dislocation: Rehab, Surgery, and the Re-Injury Question
A first shoulder dislocation raises one urgent question: will it happen again? The answer depends heavily on your age and your sport, and it shapes the whole plan.
BY ALI SHAFIEI, RPT
A shoulder dislocation is dramatic and painful, and once the joint is back in place the relief is huge. But it leaves a real question hanging: will it happen again? The honest answer depends a lot on who you are, and that answer shapes everything about how the shoulder should be managed.
What happens in a dislocation
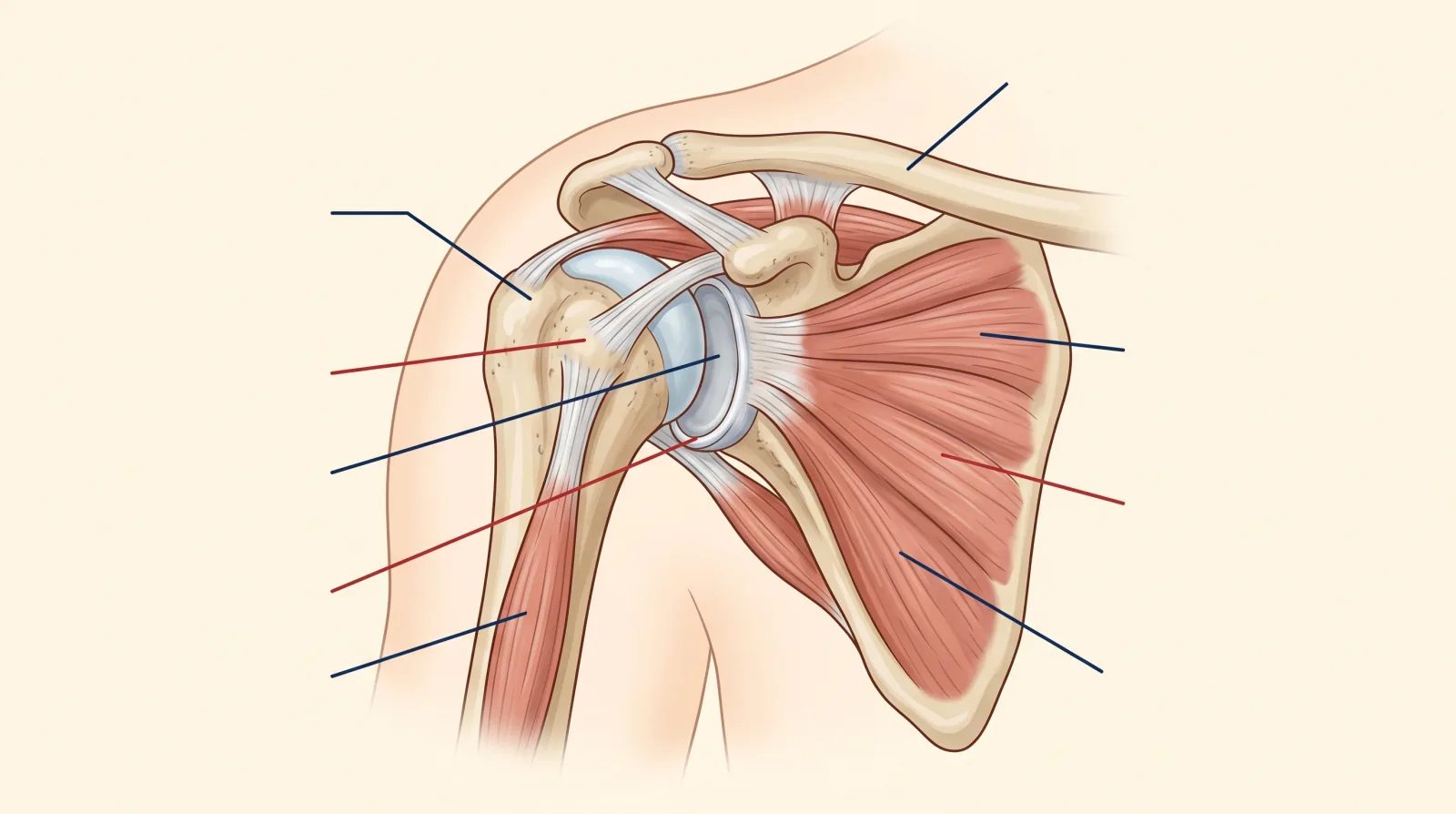
The shoulder is the most mobile joint in the body. The ball of the upper arm sits in a shallow socket, held in place by a rim of cartilage called the labrum, a capsule of ligaments, and the muscles of the rotator cuff and shoulder blade. That shallow design is what lets you reach overhead and behind your back, but it also means the joint can be forced out of position, most often forward, during a fall, a tackle, or an awkward overhead movement.
When the shoulder dislocates, it usually stretches or tears some of the structures that hold it in place. How much damage occurs, and to which structures, is part of what determines the risk of it happening again.
Age changes everything
The single biggest factor in the re-dislocation question is age. Younger people, especially teenagers and those in their twenties who play contact or overhead sports, have a high rate of dislocating the same shoulder again after a first event. Their tissues and activity demands combine to leave the joint vulnerable.
Older adults are a different story. They are much less likely to dislocate again, but more likely to have torn part of the rotator cuff during the same injury. So in an older adult, the priority shifts from preventing the next dislocation to checking for and managing a cuff tear, which connects to how we manage rotator cuff shoulder pain more generally.
This is why two people with the same diagnosis can need very different plans. The teenage rugby player and the 60-year-old who dislocated reaching for a falling box share a word, not an injury.
Sling use has changed
For years, the standard advice was to immobilize a dislocated shoulder in a sling for several weeks. That is no longer the routine recommendation for most cases. Short-term sling use for comfort in the first few days is fine, but prolonged immobilization does not reliably reduce re-dislocation and can leave the shoulder stiff and weak.
The current approach favours protecting the shoulder early, then beginning guided movement and strengthening sooner. The exact timeline still depends on the injury and is set after assessment, but the days of automatically parking every shoulder in a sling for a month are behind us.
What rehab involves
Physiotherapy after a dislocation moves through stages. First, we restore range of motion safely, avoiding the positions that put the healing structures at risk early on. Then we rebuild the strength and control of the rotator cuff and the shoulder-blade muscles, which are the dynamic stabilizers that keep the ball centred in the socket.
From there, the program progresses toward the specific demands of your life and sport. A swimmer, a climber, and a hockey player all need different end points, because their shoulders face instability in different positions. The goal throughout is not just a pain-free shoulder but a stable one that can handle load and quick movement without feeling like it might slip.
When surgery is considered
Many first dislocations are managed without surgery. Surgery enters the conversation more often for young, high-demand athletes whose re-dislocation risk is high, or when imaging shows significant structural damage to the labrum or bone that makes the joint mechanically unstable.
That decision belongs with an orthopaedic surgeon, who weighs your age, sport, imaging, and the number of dislocations. Our role is to help you get there with a clear picture, to prepare the shoulder if surgery is planned, and to lead the recovery afterward. Whether the path is conservative or surgical, structured rehab is part of it, much like the planning that goes into any post-surgical rehab.
Returning to sport
Return to sport after a dislocation is based on criteria, not the calendar. We look for full, confident range of motion, restored rotator-cuff and shoulder-blade strength, and the ability to control the shoulder in the positions your sport demands. Contact and overhead athletes return later than recreational exercisers because their shoulders face higher instability loads, and rushing that timeline is a common reason people re-dislocate.
Confidence matters too. A shoulder that is physically ready but that the athlete does not trust will be guarded and protected, which changes movement and raises injury risk elsewhere. Part of good rehab is rebuilding that trust through progressive, successful exposure to demanding positions.
When to get it assessed
If you have dislocated a shoulder, get it assessed once the acute pain has settled, even if it relocated easily and feels okay. The re-dislocation risk and the chance of a cuff tear are both invisible from the outside and both shape the plan. Waiting and hoping is the approach most likely to lead to a second dislocation.
Book a 30-minute appointment and we will assess the shoulder, factor in your age and sport, coordinate with a surgeon if that is warranted, and build a rehab plan that aims for a stable shoulder, not just a quiet one.
This article is general information about shoulder dislocations. It is not personal medical advice. A regulated practitioner can confirm whether the patterns described apply to you, and significant or recurrent instability should be assessed by a physician.
Sources
- Hovelius et al. — Nonoperative treatment of primary anterior shoulder dislocation in patients forty years of age and younger, Journal of Bone and Joint Surgery (2008)
- Kavaja et al. — Treatment after traumatic shoulder dislocation: a systematic review with a network meta-analysis, British Journal of Sports Medicine (2018)
- College of Physical Therapists of BC (CPTBC)
Share this post
Copies a ready-to-publish LinkedIn post to your clipboard and opens the LinkedIn share dialog. Paste the text into the composer and publish.

Written by
Ali Shafiei, RPTAli Shafiei — Registered Physiotherapist with 10+ years of clinical experience in musculoskeletal, neurological and sports rehabilitation. North Vancouver.
Filed under
- shoulder-dislocation
- shoulder-instability
- rehab
- return-to-sport
- north-vancouver


